
Latest posts
.
-
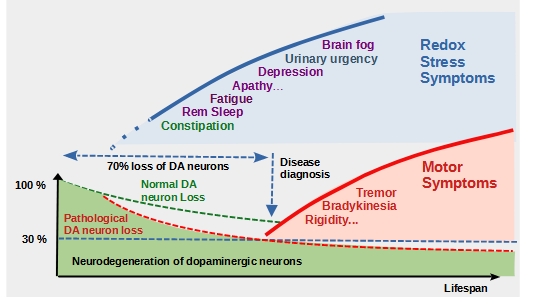
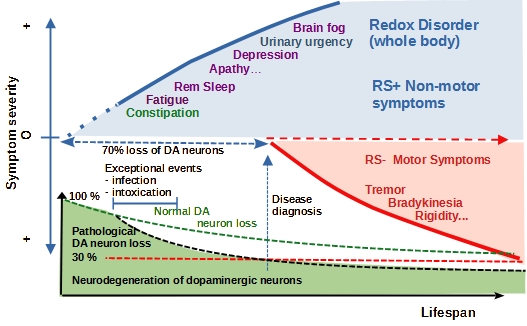
Describing Parkinson’s as a single disease is inaccurate and misleading. It is more accurate to describe Parkinson’s as two quite distinct pathologies which occur in a specific sequence, but then progress in parallel.
-
A critical guide to Parkinson’s symptoms
In this post I review the symptoms of Parkinson’s as defined by the “Idealized vision of Parkinson’s” promoted by the mainstream Parkinson’s Institutions and Charities and compare them to symptoms defined by my own observations, research and experimentation
-
What can we learn from non-motor symptoms?
Explore the connection between non-motor symptoms of Parkinson’s disease and mitochondrial dysfunction in the central nervous system, the gastrointestinal and lower urinary tracts in order to understand the impact of non-motor symptoms in Parkinson’s disease.
-
Parkinson’s for Beginners
Parkinson’s disease is diagnosed when the first motor symptoms appear. This is the beginning of the second stage of the disease when the loss of dopamine-producing neurons reaches a threshold (~70% loss), beyond which normal motor function is impaired.
-
The Redox Stress Test
A Redox Stress Test was developed to identify symptoms of diseases driven by oxidative stress. Symptom changes induced by activation of the transcription factor Nrf2, show that many non-motor symptoms are the caused by OS.
-
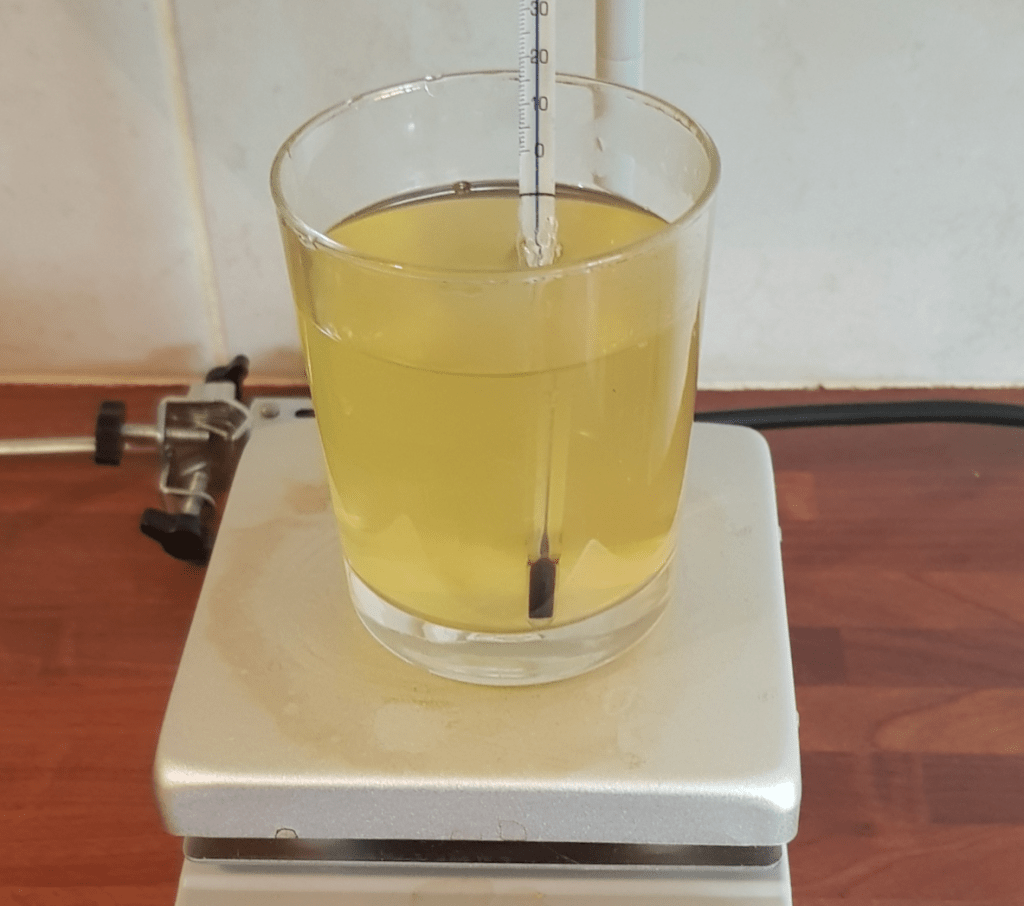
Instructions for making Broccoli Seed Tea*
Broccoli Seed Tea is not available as a commercial product. A step by step guide has been prepared to help you buy the right seeds and make Broccoli Seed Tea containing fully bioavailable sulforaphane at home. This guide is accessible…
Join 900+ subscribers
Stay in the loop with everything you need to know.
