
Latest posts
.
-
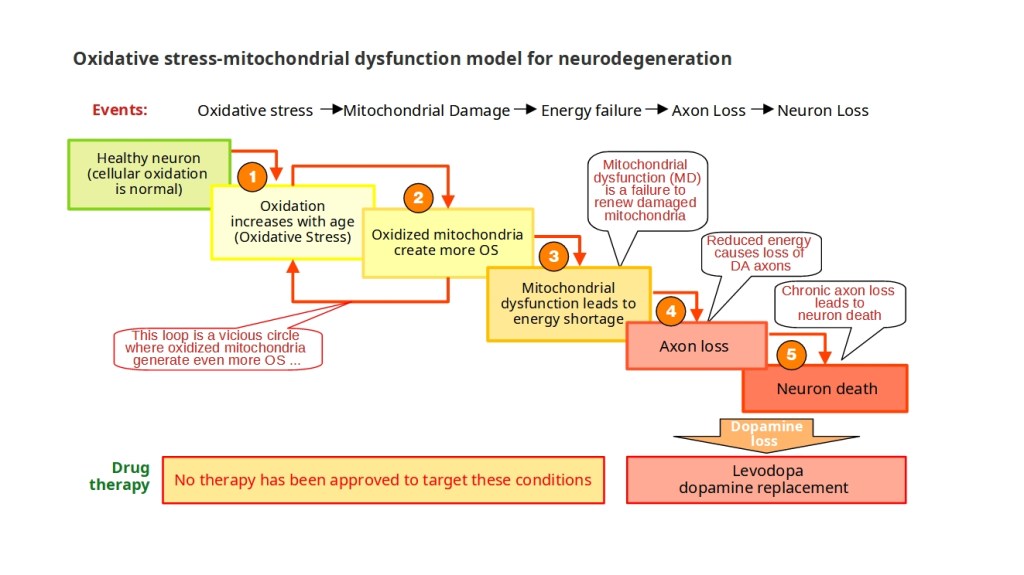
The research focuses on halting mitochondrial damage in dopamine-producing neurons. Activating Nrf2 reduces oxidative stress and mitochondrial damage, preventing a self-perpetuating cycle that reduces energy production and increases ROS levels.
-
A Scientist with Parkinson’s Disease
The story of my my five-year journey with Parkinson’s disease. It starts with the diagnosis and the dreadful declaration by the neurologist that the causes of Parkinson’s Disease remains a mystery, which is used to justify why there are currently…
-

The diagnosis
I was diagnosed with Parkinson’s disease in 2018, but I had been grappling with many of its symptoms for years before that. It all started with the loss of my sense of smell, but it was the symptoms that affected…
-
The broccoli seed tea experiment
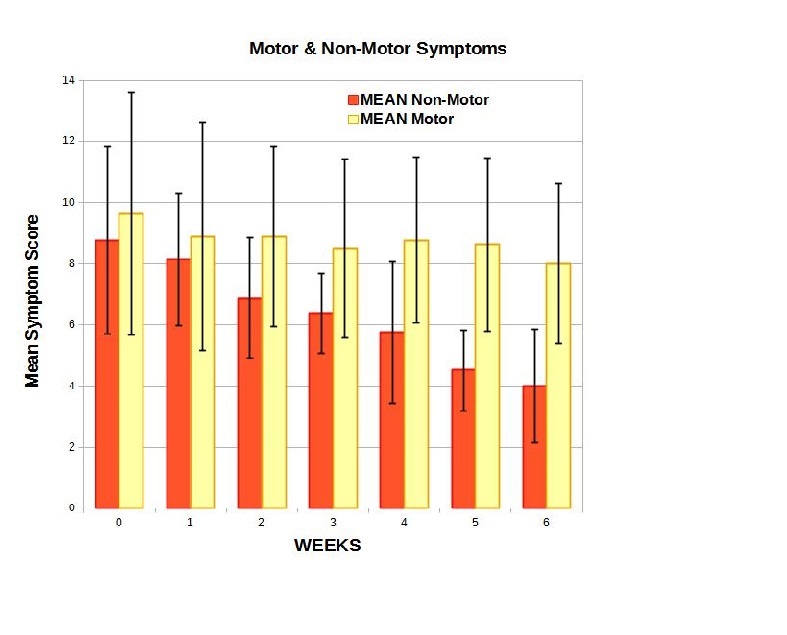
Eight coordinated studies, conducted by people with Parkinson’s, found that non-motor symptoms were significantly reduced by broccoli seed tea, while motor symptoms showed no change over the 6-week program.
-

Resetting the Redox Balance
After over a year of extensive research and experimentation, a small cohort of individuals with Parkinson’s disease effectively conducted a 6-week investigation utilizing a specially formulated Broccoli seed tea aimed at mitigating oxidative stress in neurons.
Join 900+ subscribers
Stay in the loop with everything you need to know.
